Advice on Diagnosing Plagiocephaly: A Q&A With Dr. Michael Cunningham
August 1, 2018
 Positional plagiocephaly, also known as deformational plagiocephaly or nonsynostotic plagiocephaly, is a condition in which an infant develops a flat spot on the back or side of their head.
Positional plagiocephaly, also known as deformational plagiocephaly or nonsynostotic plagiocephaly, is a condition in which an infant develops a flat spot on the back or side of their head.
While this condition is common and arguably harmless, it can be challenging to differentiate it from the more detrimental condition craniosynostosis.
Additionally, recent research has led to some misunderstanding regarding the correlation between plagiocephaly and developmental issues.
Provider News spoke with Dr. Michael Cunningham, medical director of Seattle Children’s Craniofacial Center to gather information for providers diagnosing plagiocephaly and counseling families on this condition.
How do you describe plagiocephaly to patient families?
Plagiocephaly is a flat spot on the back or side of a baby’s head. It is caused by pressure on the bones of the skull before or after birth. This usually happens because of the way a baby likes to lie in their first few months of life. Because of the “Back to Sleep” campaign, it’s almost always posterior these days. By itself, a flat spot on a young baby’s head is generally not a concern.
Families should know plagiocephaly is a benign condition. The condition is often at its worst between 2 and 4 months of age, but after 4 months it usually improves with some repositioning. If the condition seems to be getting worse after 4 months, patients should be referred to a specialist for further evaluation.
What advice do you offer to providers diagnosing plagiocephaly?
Positional plagiocephaly can look different depending on which part of the skull has a flat spot. It can be very mild and hard to see, or it can be very easy to see.
Often only the back of a baby’s head has a flat spot. Sometimes the forehead or face is also uneven. Usually the flatness is asymmetric, because babies like to rest on one side more than the other. Sometimes the flatness only affects the middle of the back of the head, if a baby tends to lie without turning their head.
Providers should check the child’s head for features like:
- Bony ridges
- Flat areas
- Uneven forehead
- Two sides of the face that do not match each other (asymmetry)
- Ears that look different from each other
I understand plagiocephaly and craniosynostosis can present similarly. How can providers tell these conditions apart?
This is an important distinction because these conditions require very different kinds of treatment. If providers are unsure, they should not hesitate to refer a patient to Children’s Craniofacial Center. Our team is experienced in looking for the signs that help us tell these conditions apart.
In this era, children with plagiocephaly almost entirely are affected on the back of their skull. However, a rare type of craniosynostosis — lambdoid synostosis — also presents with flatness in the back of the head.
The following images can help distinguish differences providers might identify: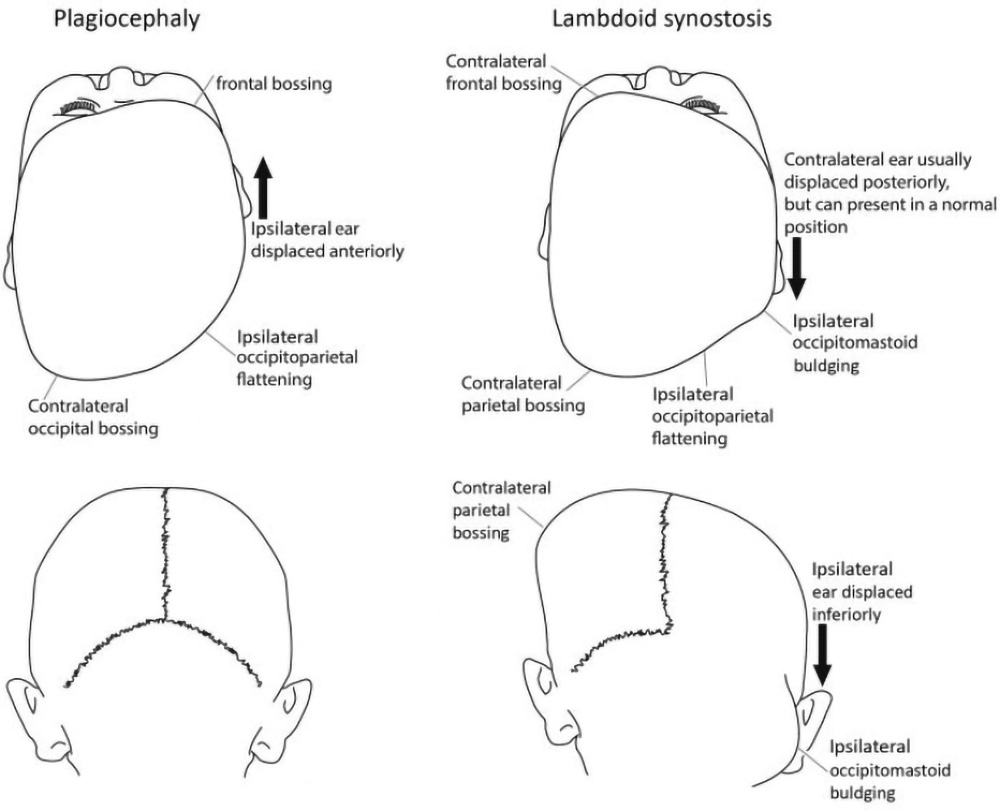
Additionally, it is worth noting that while as many as two-thirds of infants have some degree of deformational plagiocephaly, lambdoid synostosis only occurs in about one in 50,000 people.
Tell us about the link between plagiocephaly and developmental delays.
Recent studies by Children’s found increased developmental delays in infants, toddlers and preschoolers with positional plagiocephaly compared to children without positional plagiocephaly. This has been occasionally misunderstood as causation — that if a child has plagiocephaly that condition is going to cause developmental delays.
We can’t distinguish the two, but our opinion is that the correlation exists because infants who have mild delays don’t move as much, so they’re more likely to develop plagiocephaly. We believe treating plagiocephaly does not affect developmental outcomes.
However, we do think plagiocephaly may be a “marker” that could identify if a child is at risk for delayed development, so we recommend that all babies with flattened skulls be screened by their primary providers for developmental problems.
What are the risk factors of plagiocephaly that providers should be aware of?
Many things can increase the chance of positional plagiocephaly:
- Many medical problems or delayed development. These may make it harder for a baby to change positions.
- A baby tending to look in one direction. If a baby’s neck muscles become too tight on one side, it can limit how much they can move their neck. This is called torticollis. It can cause the baby to always rest on the same spot on the back of their head.
- Premature birth. The skull bones of premature babies are softer than the skulls of babies born at full term. They also tend to move their heads less often.
- Being crowded in the womb. Crowding may happen if there is more than one baby in the womb (twins or triplets). Sometimes it happens if the mother has a womb with an unusual shape or has uterine fibroids (noncancerous tumors).
- Maleness and/or having a large head. Plagiocephaly is more common in boys than girls, which may be related to head size. Children who have large heads are also more prone to plagiocephaly because they can’t lift their head and rotate easily.
Is it possible to prevent plagiocephaly?
Plagiocephaly is a cosmetic issue, so how concerned one should be is linked to how concerned one is about the shape of their child’s head. However, providers and parents should be aware of things they can do to prevent plagiocephaly.
The most important prevention tactic is to keep babies off their back when they’re awake. A healthy infant with a healthy interaction with their parents is rarely on their back for long periods when awake. They sleep on their back, but even then they actually rotate their head a lot.
Tummy time isn’t just about keeping your kid’s head from getting flat; it improves upper body strength and helps babies get up onto their arms and learn to crawl. If you have a baby who is lying flat on their back during the day when they are wide awake, they learn that the world comes to them because they are imobile. But if a baby is awake and on their stomach, they can engage in the world around them. They lift their heads up, get up on their arms and reach and crawl — all activities that lead to good developmental outcomes in terms of neuromuscular development and more.
If a child is noted to have torticollis start stretching exercises or therapy as soon as it is noted—that will help to prevent plagiocephaly or keep it from getting worse.
Providers should offer the following tips to parents:
- Always place your baby to sleep on their back. This is the safest way.
- When your baby is awake, find ways for them to play and move while on their tummy, such as:
- Choose different positions and ways for your baby to play and be held. Variety is important.
- Give your baby a lot of time sitting in laps and cuddling. When they are awake, avoid long periods lying on their back or strapped into infant seats or car seats.
- Encourage crawling, rolling, reaching, pushing, pulling, holding and grasping.
- It is OK to use strollers, car seats, infant seats, bassinets, cribs and play pens when necessary. But remember that babies need chances to move that do not happen while sitting in only one position.
What treatment options does Children’s offer for plagiocephaly?
Treatment depends on the cause, child’s age and how much their skull is affected. Options include:
- If muscle tightness limits the baby’s movement in the neck (torticollis), our team may recommend exercises or refer the patient to a physical therapist.
- If lying in the same position is the cause and the baby is 5 months or less, the most important treatment is to change the position of their head when they lie down. Our team will help parents learn to keep their baby off the flat portion of their head as much as possible. It is still important to put babies to sleep on their backs to lower the risk of sudden infant death syndrome (SIDS).
- If changing the baby’s position does not reduce the flatness and the baby is 6 months or older, a special helmet may help restore their head shape.
When should providers refer a patient to Children’s, and when should they go directly to an orthotist?
If a provider is ever uncomfortable about the diagnosis or appropriate treatment, or if the pattern, of head shape abnormality is not consistent with plagiocephaly, they should not hesitate to refer to us.
For patients who have classic head-shape abnormalities consistent with plagiocephaly, providers should feel confident referring them directly to orthotic management.
Additionally, any time a provider is inclined to image a patient they are concerned about, they should consider contacting us. We can often make a diagnosis clinically without imaging, and if there’s something about a patient’s case that’s unusual, we would be happy to see them.
We are happy to see any patient whose parents want a consultation. When a provider decides to refer to orthotics directly, insurance often requires documentation on whether the baby has been repositioned, for how long and whether the baby has undergone therapy for torticollis. There are many local orthotists that can provide helmet therapy in addition to our orthotics department here at Children’s.
What should providers tell their patients about helmet therapy?
At Seattle Children’s, we use the Starband helmet. It fits snugly on the round parts of the baby’s head but is looser on the flat parts. This gives the flat parts more room to expand as the baby’s head grows.
Babies wear the helmet 23 hours each day. How long treatment lasts depends on the baby’s age and how severe the flatness is. Often children wear the helmet for at least 4 to 5 months.